|
Overview
 A person with flat feet (fallen arches) has low arches or no arches at all. Most cases don't cause problems and treatment isn't usually needed. The arch, or instep, is the inside part of the foot that's usually raised off the ground when you stand, while the rest of the foot remains flat on the ground. Most people have a noticeable space on the inner part of their foot (the arch). The height of the arch varies from person to person. Causes Over-pronation is a common biomechanical problem that occurs when the arches collapse while walking or standing. This condition hampers our natural walking pattern, causing an imbalance, and leading to wear and tear in other parts of the body with every step we take. Whether you suffer from over-pronation like most of the population, or you have a true flat foot, in both cases your poor walking pattern may contribute to a range of different complaints. As we age, poor aligment of the feet causes very common conditions such as heel pain or knee pain. Over-pronation has different causes. Obesity, pregnancy, age or repetitive pounding on a hard surface can weaken the arch, leading to over-pronation. Over-pronation is also very common with athletes, especially runners, who most of them nowadays use orthotics inside their shoes. Symptoms Fallen arches symptoms may include the following. Being unable to slip fingers underneath arches. Inwards rolling of foot and ankle when running. Knee problems due to lack of support from feet. Diagnosis Runners are often advised to get a gait analysis to determine what type of foot they have and so what kind of running shoe they require. This shouldn?t stop at runners. Anyone that plays sports could benefit from this assessment. Sports shoes such as football boots, astro trainers and squash trainers often have very poor arch support and so for the 60-80% of us who do overpronate or have flat feet they are left unsupported. A change of footwear or the insertion of arch support insoles or orthotics can make a massive difference to your risk of injury, to general aches and pains and even to your performance. Is flat footedness genetic? Non Surgical Treatment Custom orthotics are specially designed insoles, which are made for your by prescription. This is done by taking a plaster cast of the foot in its neutral position and is then sent to a laboratory, with your prescription to be made to your exact specifications. The insole then correctly aligns your foot and as a result your body. This will relieve abnormal strain of tissues and structures which can cause pain. For less severe mal-alignments or for sports use a wide variety of temporary insoles. Surgical Treatment  Rarely does the physician use surgery to correct a foot that is congenitally flat, which typically does not cause pain. If the patient has a fallen arch that is painful, though, the foot and ankle physicians at Midwest Orthopaedics at Rush may perform surgery to reconstruct the tendon and "lift up" the fallen arch. This requires a combination of tendon re-routing procedures, ligament repairs, and bone cutting or fusion procedures. Prevention Orthotic inserts, either prescribed or bought over the counter, can help keep the arches fixed into position, but always wear them as although they support, they don?t strengthen, which is why some experts reccomend avoiding them. Gait analysis at a run specialist can help to diagnose overpronation and flat feet. Most brands produce shoes that will give support and help to limit the negative effects of a poor gait on the rest of the body. Barefoot exercises, such as standing on a towel and making fists with the toes, can help to strengthen the arches. Start easy and build up the reps to avoid cramping. Short barefoot running sessions can help take pressure off the arches by using the natural elasticity of the foot?s tendons to take impact and build strength to help prevent flat feet. These should be done on grass for only a few minutes at a time. After Care Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low. Overview
 Your foot is made up of 26 bones, 33 joints, and more than 100 tendons. The heel is the largest bone in your foot. If you overuse or injure your heel, you may experience heel pain. This can range from mild to disabling. In many cases, if you have heel pain, you will need a doctor to diagnose the cause. Causes One of the most common heel pain causes is a condition called plantar fasciitis. The tendons, ligaments, muscles, and joints in the feet all work together to allow you to move your feet to walk or run. When the plantar fascia, or the arch of the foot, is overused or injured, pain is felt in the heel. The most common heel pain causes include plantar fasciitis, Achilles tendonitis, Bursitis, Fibromyalgia, Bone fracture, Heel spurs, Arthritis, Tarsal tunnel syndrome, Sever?s Disease. Symptoms See your doctor as soon as possible if you experience severe pain accompanied by swelling near your heel. There is numbness or tingling in the heel, as well as pain and fever. There is pain in your heel as well as fever. You are unable to walk normally. You cannot bend your foot downwards. You cannot stand with the backs of the feet raised (you cannot rise onto your toes). You should arrange to see a doctor if the heel pain has persisted for more than one week. There is still heel pain when you are not standing or walking. Diagnosis The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel. Non Surgical Treatment Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence. Surgical Treatment With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick. deelsonheels Prevention  Make sure you wear appropriate supportive shoes. Don't over-train in sports. Make sure you warm up, cool down and undertake an exercise regime that helps maintain flexibility. Manage your weight, obesity is a factor in causing plantar fasciitis. Avoid walking and running on hard surfaces if you are prone to pain. You should follow the recognized management protocol "RICED" rest, ice, compression, elevation and diagnosis. Rest, keep off the injured ankle as much as possible. Ice, applied for 20 minutes at a time every hour as long as swelling persists. Compression, support the ankle and foot with a firmly (not tightly) wrapped elastic bandage. Elevation, keep foot above heart level to minimize bruising and swelling. Diagnosis. Consult a medical professional (such as a Podiatrist or doctor) especially if you are worried about the injury, or if the pain or swelling gets worse. If the pain or swelling has not gone down significantly within 48 hours, also seek treatment. An accurate diagnosis is essential for proper rehabilitation of moderate to severe injuries. Overview
Leg length discrepancy is a condition where the length of one leg is different than the other (shorter or longer) because of either or both a functional (muscle/posture) or structural (bone/cartilage) abnormality. In the specific a functional leg length occurs when your legs are the same, but another condition such as pelvic tilt or piriformis shortening creates the appearance of one leg being longer or shorter than the other. A structural leg length inequality it means that there is a true difference. Osteopaths, chiropractors and physiotherapist should be able to determine the degree of leg length inequality using visual inspection and manual tests.  Causes LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio. Symptoms The symptoms of limb deformity can range from a mild difference in the appearance of a leg or arm to major loss of function of the use of an extremity. For instance, you may notice that your child has a significant limp. If there is deformity in the extremity, the patient may develop arthritis as he or she gets older, especially if the lower extremities are involved. Patients often present due to the appearance of the extremity (it looks different from the other side). Diagnosis Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all. Non Surgical Treatment Internal heel lifts: Putting a simple heel lift inside the shoe or onto a foot orthotic has the advantage of being transferable to many pairs of shoes. It is also aesthetically more pleasing as the lift remains hidden from view. However, there is a limit as to how high the lift can be before affecting shoe fit. Dress shoes will usually only accommodate small lifts (1/8"1/4") before the heel starts to piston out of the shoe. Sneakers and workboots may allow higher lifts, e.g., up to 1/2", before heel slippage problems arise. External heel lifts: If a lift of greater than 1/2" is required, you should consider adding to the outsole of the shoe. In this way, the shoe fit remains good. Although some patients may worry about the cosmetics of the shoe, it does ensure better overall function. Nowadays with the development of synthetic foams and crepes, such lifts do not have to be as heavy as the cork buildups of the past. External buildups are not transferable and they will wear down over time, so the patient will need to be vigilant in having them repaired. On ladies' high-heel shoes, it may be possible to lower one heel and thereby correct the imbalance.  what is a functional leg length discrepancy? Surgical Treatment Surgical treatments vary in complexity. Sometimes the goal of surgery is to stop the growth of the longer limb. Other times, surgeons work to lengthen the shorter limb. Orthopedic surgeons may treat children who have limb-length conditions with one or a combination of these surgical techniques. Bone resection. An operation to remove a section of bone, evening out the limbs in teens or adults who are no longer growing. Epiphyseal stapling. An operation to slow the rate of growth of the longer limb by inserting staples into the growth plate, then removing them when the desired result is achieved. Epiphysiodesis. An operation to slow the rate of growth of the longer limb by creating a permanent bony ridge near the growth plate. Limb lengthening. A procedure (also called distraction osteogenesis or the Ilizarov procedure) that involves attaching an internal or external fixator to a limb and gradually pulling apart bone segments to grow new bone between them. There are several ways your doctor can predict the final LLD, and thus the timing of the surgery. The easiest way is the so-called Australian method, popularised by Dr. Malcolm Menelaus, an Australian orthopedic surgeon. According to this method, growth in girls is estimated to stop at age 14, and in boys at age 16 years. The femur grows at the rate of 10 mm. a year, and the upper tibia at the rate of 6 mm. a year. Using simple arithmetic, one can get a fairly good prediction of future growth. This of course, is an average, and the patient may be an average. To cut down the risk of this, the doctor usually measures leg length using special X-ray technique (called a Scanogram) on three occasions over at least one year duration to estimate growth per year. He may also do an X-ray of the left hand to estimate the bone age (which in some cases may differ from chronological age) by comparing it with an atlas of bone age. In most cases, however, the bone age and chronological age are quite close. Another method of predicting final LLD is by using Anderson and Green?s remaining growth charts. This is a very cumbersome method, but was till the 1970?s, the only method of predicting remaining growth. More recently, however, a much more convenient method of predicting LLD was discovered by Dr. Colin Moseley from Montreal. His technique of using straight line graphs to plot growth of leg lengths is now the most widely used method of predicting leg length discrepancy. Whatever method your doctor uses, over a period of one or two years, once he has a good idea of the final LLD, he can then formulate a plan to equalize leg lengths. Epiphyseodesis is usually done in the last 2 to 3 years of growth, giving a maximum correction of about 5 cm. Leg lengthening can be done at any age, and can give corrections of 5 to10 cm., or more. Overview
 This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton. This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton.Causes A Morton's neuroma commonly occurs due to repetitive weight bearing activity (such as walking or running) particularly when combined with tight fitting shoes or excessive pronation of the feet (i.e. "flat-feet"). The condition is also more common in patients with an unstable forefoot allowing excessive movement between the metatarsal bones. A Morton's neuroma can also occur due to certain foot deformities, trauma to the foot, or the presence of a ganglion or inflamed bursa in the region which may place compressive forces on the nerve. Symptoms Patients will feel pain that worsens with walking, particularly when walking in shoes with thin soles or high heels. Also, anything that squeezes the metatarsal heads together may aggravate symptoms, such as narrow shoes. A patient may feel the need to remove the shoe and rub the foot to soothe the pain. Diagnosis The clinical symptoms should quickly lead your doctor to suspect a neuroma. When examined, the doctor may feel a "click" which is known as Mulder's sign. There may be tenderness in the interspace. The metatarsal bones will also be examined both clinically (and often with an xray). Tenderness at one of the metatarsal bones can suggest an overstress reaction (pre-stress fracture or stress fracture) in the bone. An ultrasound scan can confirm the diagnosis and is a less expensive and at this time, at least as sensitive a test as an MRI. An x-ray does not show neuromas, but can be useful to "rule out" other causes of the pain. Non Surgical Treatment In developing a treatment plan, your foot and ankle surgeon will first determine how long you?ve had the neuroma and evaluate its stage of development. Treatment approaches vary according to the severity of the problem. For mild to moderate neuromas, treatment options may include Padding techniques provide support for the metatarsal arch, thereby lessening the pressure on the nerve and decreasing the compression when walking. Placing an icepack on the affected area helps reduce swelling. Custom orthotic devices provided by your foot and ankle surgeon provide the support needed to reduce pressure and compression on the nerve. Activities that put repetitive pressure on the neuroma should be avoided until the condition improves. Wear shoes with a wide toe box and avoid narrow-toed shoes or shoes with high heels. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Treatment may include injections of cortisone, local anesthetics or other agents.  Surgical Treatment Should the problem have progressed beyond the point where these measures are sufficient, the podiatric professional may recommend surgery. This procedure involves excision of the involved nerve mass. This will relieve the pain. Many patients report permanent numbness in the spot formerly affected by the neuroma, but prefer it to the pain. Most surgeries are successful; unfortunately, there are cases where the patient suffers another neuroma, sometimes in or near the same spot as before. A podiatric professional can explain the statistics of recurrence in various cases. If you suspect a neuroma, don?t wait for it to get better on its own. The earlier the diagnosis, the higher the likelihood that it can be treated with conservative measures. Don?t think that foot pain of any kind is inevitable, either, even if it runs in your family. Prevention Wearing shoes that fit properly and that have plenty of room in the toe area may help prevent Morton's neuroma.  Overview OverviewThe term Hammer toes describes three unique contracture deformities of the toes. The deformities differ by the location of contracture in each joint of the toe. The three deformities include hammer toe, claw toe and mallet toe. Hammer toes may be flexible or rigid. Hammer toes are most common on the lesser toes (2-5) and may affect one or more toes simultaneously. Hallux malleus is the term used to described a hammer toe of the great toe. Hallux malleus is often found as an isolated foot problem. Hammer toes are found equally in men and women. The onset of hammer toes is between the ages of 30 and 80 years of age. Causes Hammer toe is commonly caused by wearing shoes that are too narrow, tight or short on a regular basis. By doing so, your toe joints are forced into odd position. Over time, the tendons and muscles in your toe become shorter and cause it to bend. You can suffer a hammer toe if you have diabetes and the disease is worsening. If this occurs, you should contact your doctor right away. Arthritis can also cause hammer toes. Because your toe muscles get out of balance when you suffer from this joint disorder, tendons and joints of your toes are going to experience a lot of pressure.  Symptoms Well-developed hammertoes are distinctive due to the abnormal bent shape of the toe. However, there are many other common symptoms. Some symptoms may be present before the toe becomes overly bent or fixed in the contracted position. Often, before the toe becomes permanently contracted, there will be pain or irritation over the top of the toe, particularly over the joint. The symptoms are pronounced while wearing shoes due to the top of the toe rubbing against the upper portion of the shoe. Often, there is a significant amount of friction between the toe and the shoe or between the toe and the toes on either side of it. The corns may be soft or hard, depending on their location and age. The affected toe may also appear red with irritated skin. In more severe cases, blisters or open sores may form. Those with diabetes should take extra care if they develop any of these symptoms, as they could lead to further complications. Diagnosis Hammertoes are progressive, they don?t go away by themselves and usually they will get worse over time. However, not all cases are alike, some hammertoes progress more rapidly than others. Once your foot and ankle surgeon has evaluated your hammertoes, a treatment plan can be developed that is suited to your needs. Non Surgical Treatment There is a variety of treatment options for hammertoe. The treatment your foot and ankle surgeon selects will depend upon the severity of your hammertoe and other factors. A number of non-surgical measures can be undertaken. Padding corns and calluses. Your foot and ankle surgeon can provide or prescribe pads designed to shield corns from irritation. If you want to try over-the-counter pads, avoid the medicated types. Medicated pads are generally not recommended because they may contain a small amount of acid that can be harmful. Consult your surgeon about this option. Changes in shoewear. Avoid shoes with pointed toes, shoes that are too short, or shoes with high heels, conditions that can force your toe against the front of the shoe. Instead, choose comfortable shoes with a deep, roomy toe box and heels no higher than two inches. Orthotic devices. A custom orthotic device placed in your shoe may help control the muscle/tendon imbalance. Injection therapy. Corticosteroid injections are sometimes used to ease pain and inflammation caused by hammertoe. Medications. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Splinting/strapping. Splints or small straps may be applied by the surgeon to realign the bent toe. Surgical Treatment The technique the surgeon applies during the surgery depends on how much flexibility the person's affected toes still retain. If some flexibility has still been preserved in their affected toes, the hammer toes might be corrected through making a small incision into the toe so the surgeon can manipulate the tendon that is forcing the person's toes into a curved position. If, however, the person's toes have become completely rigid, the surgeon might have to do more than re-aligning the person's tendons. Some pieces of bone may have to be removed so the person's toe has the ability to straighten out. If this is the case, some pins are attached onto the person's foot afterwards to fix their bones into place while the injured tissue heals.
Overview
 The classic bunion is a bump on the side of the great toe joint. This bump represents an actual deviation of the 1st metatarsal. In addition, there is also deviation of the great toe toward the second toe. In severe cases, the great toe can either lie above or below the second toe. The classic bunion is a bump on the side of the great toe joint. This bump represents an actual deviation of the 1st metatarsal. In addition, there is also deviation of the great toe toward the second toe. In severe cases, the great toe can either lie above or below the second toe.Causes Although bunions tend to run in families, it is the foot type that is passed down-not the bunion. Parents who suffer from poor foot mechanics can pass their problematic foot type on to their children, who in turn are prone to developing bunions. The abnormal functioning caused by this faulty foot development can lead to pressure being exerted on and within the foot, often resulting in bone and joint deformities such as bunions and hammertoes. Symptoms Bunions or hallux valgus tend to give pain predominantly from the metatarsal head on the inner border of the foot. The bunion tends to be painful mainly when in enclosed shoes and so is often more symptomatic in winter. As the front part of the foot splays and the great toe moves across towards the 2nd toe a bunion can also produce pain from the 2nd toe itself. The pain which a bunion produces on the 2nd toe is either due to direct rubbing between the great toe and the 2nd toe, a hammer toe type deformity produced due to crowding of the 2nd toe by the bunion and the 3rd toe.The hammer toe will either be painful from its top aspect where it rubs directly on shoe wear or its under surface in the area of the 2nd metatarsal head. This is made prominent and pushed to the sole of the foot by the 2nd toe rising upwards and driving the metatarsal head downwards. Diagnosis Looking at the problem area on the foot is the best way to discover a bunion. If it has the shape characteristic of a bunion, this is the first hint of a problem. The doctor may also look at the shape of your leg, ankle, and foot while you are standing, and check the range of motion of your toe and joints by asking you to move your toes in different directions A closer examination with weight-bearing X-rays helps your doctor examine the actual bone structure at the joint and see how severe the problem is. A doctor may ask about the types of shoes you wear, sports or activities (e.g., ballet) you participate in, and whether or not you have had a recent injury. This information will help determine your treatment. Non Surgical Treatment The choice of treatment for a bunion lies between non-operative (conservative) and operative treatment. Conservative treatment for a bunion means either wearing wider fitting shoes or shoes with softer leather or using some form of a spacer between the big toe and 2nd toe (or alternatively some form of splint to keep the great toe away from the 2nd toe). The spacers or splintage may apparently straighten the bunion but they make no difference to the width of the foot, and the splaying of the 1st and 2nd metatarsals which occur with a bunion deformity. Therefore this type of treatment will not improve the main pain in a bunion which occurs due to the width of the forefoot. An arch type support orthotic may be useful if a bunion is associated with a flatter foot. If you have a bunion this is however just one other thing to get into a shoe with an already wide foot.  Surgical Treatment Bunion Surgery Is Not Cosmetic Surgery. Bunions may not be pretty, but cosmetic deformity is not a good reason to perform surgery. There are too many potential complications to perform a bunion surgery simply for cosmetic reasons. Patients Must Have Realistic Expectations. Bunion surgery can be helpful at relieving pain, but patients should not expect to have "normal" feet after surgery. In one study, a leading researcher on foot problems such as bunions, found that 1/3 of his patients could not wear the type of shoe they desired prior to surgery. The Foot Width Change Is Small. Bunion surgery decreases the width of the forefoot by about 1/8 of an inch. That's not much! That is the reason why even after surgery, most patients will not be wearing slender shoes. Surgery can be an excellent treatment option for patients with problems from their bunions. That said, patients must understand this is a procedure that has potential complications and a lengthy rehabilitation. The patients who tend to be unsatisfied with bunion surgery are those patients who are having surgery done to allow them to have normal looking feet or allow them to wear slim shoes. If that sounds like your motivation, think long and hard about surgery. Surgery should be reserved for those patients who have significant pain, and are unable to correct the problem with adaptive footwear. Overview
The foot and ankle complex needs to pronate to make the muscles of the hips and legs work correctly. Many muscles that originate from the pelvis attach to both the upper and lower leg. For example, the gluteus maximus and tensor fascia latae (TFL) attach to the outside of the lower leg via the iliotibial band, while the abductors attach to the outside of the femur. When the foot pronates, the whole leg rotates inward toward the center line of the body. This inward rotation pulls the attachment of the glutes, TFL and abductors away from the origin of these muscles up on the pelvis which creates tension. Similarly, the muscles of the lower leg such as the peroneals, tibialis anterior and tibialis posterior originate on the lower leg and attach to the underside of the foot. When the foot flattens out, as it does in pronation, this pulls the insertion of these muscles away from their origin on the tibia. This action also creates tension in the muscles.  Causes Flat feet don't automatically mean you have a problem. The problem can be divided into a flexible flat foot or rigid flat foot. The rigid flat foot is one that does not change shape when the foot becomes weight bearing. i.e. it does not go through the excessive motion of pronation. Generally speaking this foot does not provide too many problems. The flexible flat foot is the type that when it becomes weight bearing the foot and ankle tends to roll in (pronates) too far. This type of person will often say I have great arches but when I stand up much of this arch disappears as the foot excessively pronates When the foot is excessively pronating and causing problems like sore ankles, feet or knees when standing or exercising then arch support is extremely important to restore the foot structure. Symptoms When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly. Diagnosis To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.  Non Surgical Treatment Wear shoes with straight or semicurved lasts. Motion-control or stability shoes with firm, multidensity midsoles and external control features that limit pronation are best. Over-the-counter orthotics or arch supports can help, too. You know you are making improvements when the wear pattern on your shoes becomes more normal. Overpronation causes extra stress and tightness to the muscles, so do a little extra stretching. Surgical Treatment HyProCure implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%. Overview
Sever?s disease is a painful condition of the heel affecting children, usually at the beginning of the growth spurt in early puberty. It is caused by inflammation at the growth plate at the back of the heel, adjacent to the Achilles tendon attachment. This is one of the most common causes of heel pain in school-aged children. Physically active children aged between eight and fourteen years old are most at risk of developing pain from Sever?s disease. It is common among children involved in soccer, little athletics, gymnastics, basketball and netball but can affect children involved in any running or jumping activity. Boys seem to be more commonly affected than girls. Causes Sever?s disease is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves a lot of heel movement. It can be associated with starting a new sport, or the start of a new season. Children who are going through adolescence are also at risk of getting it because the heel bone grows quicker than the leg. Too much weight bearing on the heel can also cause it, as can excessive traction since the bones and tendons are still developing. It occurs more commonly in children who over-pronate, and involves both heels in more than half of patients. Symptoms Symptoms include complaints of pain or tenderness in the heel (or heels), discomfort when heel is squeezed, limping, and more severe pain after walking, running or playing sports. Sever?s disease is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves lots of heel movements and hard shoes such as cleats. It can be associated with starting a new sport, or the start of a new season. It occurs more commonly in children who pronate (feet roll inward), and involves both heels in more than half of patients. Diagnosis Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain. Non Surgical Treatment Treatment may consist of one or more of the following. Elevating the heel. Stretching hamstring and calf muscles 2-3 times daily. Using R.I.C.E. (Rest, Ice, Compression, Elevation). Foot orthotics. Medication. Physical therapy. Icing daily (morning). Heating therapy. Open back shoe are best and avoid high heel shoe. The Strickland Protocol has shown a positive response in patients with a mean return to sport in less than 3 weeks. Further research into the anatomical and biomechanical responses of this protocol are currently being undertaken. Prevention As with all overuse injuries, it is important to warm up sufficiently before you exercise and warm down afterwards. You should build up any alterations in the intensity of your training gradually, and never continue exercising with weakened or fatigued muscles. Replace any worn or tattered shoes, as in this condition they become useless for absorbing shock and protecting the feet.
Overview
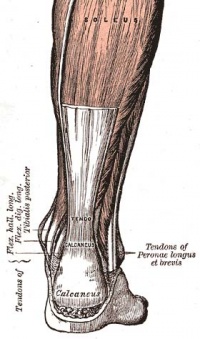 The Achilles tendon is the soft tissue located in the heel which connects calf muscle to the heel bone allowing the body to perform certain activities such as rising on the tip toes and pushing off when running or walking. Achilles tendon tears occur when the tendon becomes torn through excessive pressure put on the area which the tendon is unable to withstand. Tears are most commonly found when suddenly accelerating from a standing position and therefore is often seen in runners and athletes involved in racquet sports. A tear can also occur when a continuous force is being put on the heel through prolonged levels of activity and overuse however this can also occur as a result of sudden impact or force to the area common in contact sports such as rugby and hockey. Although Achilles tendon tears can range in their severity, a rupture is the most serious form of tear and involves a completely torn tendon. This injury is more common in patients in their 30?s and 40?s. The Achilles tendon is the soft tissue located in the heel which connects calf muscle to the heel bone allowing the body to perform certain activities such as rising on the tip toes and pushing off when running or walking. Achilles tendon tears occur when the tendon becomes torn through excessive pressure put on the area which the tendon is unable to withstand. Tears are most commonly found when suddenly accelerating from a standing position and therefore is often seen in runners and athletes involved in racquet sports. A tear can also occur when a continuous force is being put on the heel through prolonged levels of activity and overuse however this can also occur as a result of sudden impact or force to the area common in contact sports such as rugby and hockey. Although Achilles tendon tears can range in their severity, a rupture is the most serious form of tear and involves a completely torn tendon. This injury is more common in patients in their 30?s and 40?s.Causes Often the individual will feel or hear a pop or a snap when the injury occurs. There is immediate swelling and severe pain in the back of the heel, below the calf where it ruptures. Pain is usually severe enough that it is difficult or impossible to walk or take a step. The individual will not be able to push off or go on their toes. Symptoms Typically patients present with sudden onset of pain and swelling in the achilles region, often accompanied by a audible snap during forceful dorsiflexion of the foot. A classic example is that of an unfit 'weekend warrior' playing squash. If complete a defect may be felt and the patient will have only minimal plantar flexion against resistance. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if it has ruptured completely. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order an ultrasound or MRI scan. These painless procedures create images of the tissues of your body. Non Surgical Treatment Not every torn Achilles tendon needs an operation. Recent studies have shown that even a conservative treatment, i.e. immobilizingt the leg can lead to satisfactory healing successes. This requires, however, that the patient is fitted with a cast (immobilization splint) and/or a special boot for a period of approximately 6 - 8 weeks. After that, the boot must be worn during the day for about two more weeks. An intensive physiotherapy will start after about six weeks to train the calf muscles so that the initial coordination can be restored. Running training on flat ground can be started again after another 10 - 12 weeks. Studies show that the danger of a recurring torn tendon is higher after a conservative treatment opposed to an operative treatment. Depending on the type of treatment, about 10 - 15 percent of those affected can expect at some point to again suffer from a tear of the Achilles tendon. Moreover, in the non-operated cases, we see more often a significant permanent weakness of the footprint, particularly restricting the ability to participate in sports.  Surgical Treatment Thanks to a new surgical technique, operative procedures are often more beneficial.The operative treatment of Achilles tendon ruptures has significantly changed in recent years. The objective today is to connect the torn tendons using modern suture and possibly adhesive materials. Through small surgical incisions the ends of the torn tendon are surgically exposed, and sutures are used to tie the ends permanently together. Thus, the operated repaired tendon is again resilient within a reasonable time. The cast treatment and walking on crutches required in the past, is with this procedure usually not necessary. Instead, functional treatment following the surgery involves wearing a special boot, meaning that the patient can put weight onto the operated leg again within a few days after surgery. Physical therapy training will start immediately following the operation. The philosophy behind such an early functional treatment is that tissue adequately adapts to stress and thus accelerates the healing process. For the patient, the modern surgical treatment of an Achilles tendon rupture has the distinct advantage that no prolonged hospital stay is necessary. Hospital stay usually lasts only a few days. Using crutches, patients can return to work soon after the surgery.
Overview
A painful flat foot, or adult acquired flatfoot deformity, is a progressive collapsing of the arch of the foot that occurs as the posterior tibial tendon becomes insufficient due to various factors. Early stages may present with only pain along the posterior tibial tendon whereas advanced deformity usually results in arthritis and rigidity of the rearfoot and ankle.  Causes There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. Symptoms The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle. Diagnosis It is of great importance to have a full evaluation, by a foot and ankle specialist with expertise in addressing complex flatfoot deformities. No two flat feet are alike; therefore, "Universal" treatment plans do not exist for the Adult Flatfoot. It is important to have a custom treatment plan that is tailored to your specific foot. That starts by first understanding all the intricacies of your foot, through an extensive evaluation. X-rays of the foot and ankle are standard, and MRI may be used to better assess the quality of the PT Tendon. Non surgical Treatment Nonoperative treatment of posterior tibial tendon dysfunction can be successful with the Arizona AFO brace, particularly when treatment is initiated in the early stages of the disease. This mandates that the orthopedist has a high index of suspicion when evaluating patients to make an accurate diagnosis. Although there is a role for surgical management of acquired flat feet, a well-fitted, custom-molded leather and polypropylene orthosis can be effective at relieving symptoms and either obviating or delaying any surgical intervention. In today's climate of patient satisfaction directed health care, a less invasive treatment modality that relieves pain may prove to be more valuable than similar pain relief that is obtained after surgery. Questions regarding the long-term results of bracing remain unanswered. Future studies are needed to determine if disease progression and arthrosis occur despite symptomatic relief with a brace. Furthermore, age- and disease stage-matched control groups who are randomized to undergo surgery or bracing are necessary to compare these different treatment modalities.  Surgical Treatment If conservative treatment fails to provide relief of pain and disability then surgery is considered. Numerous factors determine whether a patient is a surgical candidate. They include age, obesity, diabetes, vascular status, and the ability to be compliant with post-operative care. Surgery usually requires a prolonged period of nonweightbearing immobilization. Total recovery ranges from 3 months to one year. Clinical, x-ray, and MRI examination are all used to select the appropriate surgical procedure. |
